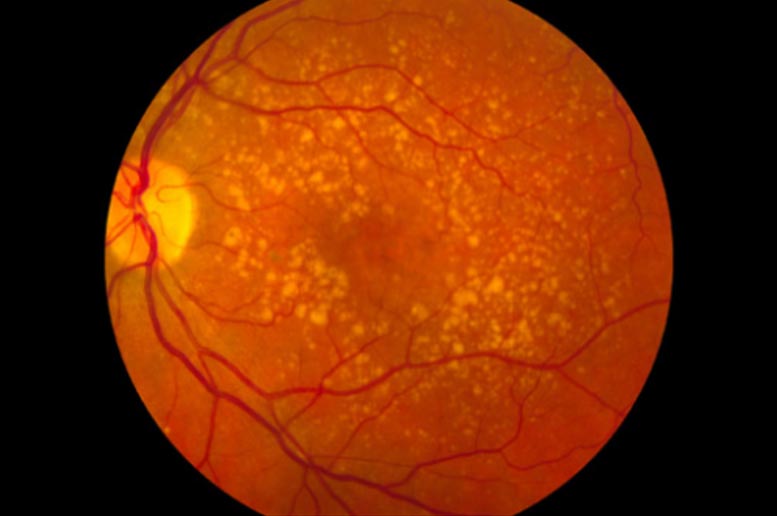
Macular degeneration, also known as age-related macular degeneration (AMD or ARMD), is a medical condition which may result in blurred or no vision in the center of the visual field.
One of the immune system’s oldest branches, called complement, may be influencing the severity of COVID-19 disease, according to a new study from researchers at Columbia University Irving Medical Center.
Among other findings linking complement to COVID, the researchers found that people with age-related macular degeneration — a disorder caused by overactive complement — are at greater risk of developing severe complications and dying from COVID.
The connection with complement suggests that existing drugs that inhibit the complement system could help treat patients with severe disease.
The study was published today (August 3, 2020) in Nature Medicine.
The authors also found evidence that clotting activity is linked to COVID severity and that mutations in certain complement and coagulation genes are associated with hospitalization of COVID patients.
“Together these results provide important insights into the pathophysiology of COVID-19 and paint a picture for the role of complement and coagulation pathways in determining clinical outcomes of patients infected with SARS-CoV-2,” says Sagi Shapira, PhD, MPH, who led the study with Nicholas Tatonetti, PhD, both professors at Columbia University Vagelos College of Physicians and Surgeons.
Findings Stem from Study of Coronavirus Mimicry
The idea to investigate the role of coagulation and complement in COVID began with a sweeping survey of viral mimicry across all viruses on earth — over 7,000 in all.
“Viruses have proteins that can mimic certain host proteins to trick the host’s cells into aiding the virus with completing its life cycle,” Shapira says. “Beyond the fundamental biological questions that we were interested in addressing, based on our previous work and the work of others, we suspected that identifying those mimics could provide clues about how viruses cause disease.”
Coronaviruses, the survey found, are masters of mimicry, particularly with proteins involved in coagulation and proteins that make up complement, one of the oldest branches of the human immune system.
Complement proteins work a bit like antibodies and help eliminate pathogens by sticking to viruses and bacteria and marking them for destruction. Complement can also increase coagulation and inflammation in the body. “Unchecked, these systems can also be quite detrimental,” says Shapira.
“The new coronavirus — by mimicking complement or coagulation proteins — might drive both systems into a hyperactive state.”
Macular Degeneration Associated with Greater COVID Mortality
If complement and coagulation influence severity of COVID, people with pre-existing hyperactive complement or coagulation disorders should be more susceptible to the virus.
That led Shapira and Tatonetti to look at COVID patients with macular degeneration, an eye disease caused by overactive complement, as well as common coagulation disorders like thrombosis and hemorrhage.
Among 11,000 COVID-19 patients who came to Columbia University Irving Medical Center with suspected COVID-19, the researchers found that over 25% of those with age-related macular degeneration died, compared to the average mortality rate of 8.5%, and roughly 20% required intubation. The greater mortality and intubation rates could not be explained by differences in the age or sex of the patients.
“Complement is also more active in obesity and diabetes,” Shapira says, “and may help explain, at least in part, why people with those conditions also have a greater mortality risk from COVID.”
People with a history of coagulation disorders also were at increased risk of dying from COVID infection.
Coagulation and Complement Pathways Activated
The researchers then examined how gene activity differed in people infected with the coronavirus.
That analysis revealed a signature in COVID-infected patients indicating that the virus engages and induces robust activation of the body’s complement and coagulation systems.
“We found that complement is one of the most differentially expressed pathways in SARS-CoV-2 infected patients,” Tatonetti says. “As part of the immune system, you would expect to see complement activated, but it seems over and above what you’d see in other infections like the flu.”
Some Coagulation and Complement Genes are Associated with Hospitalization
More evidence linking severe COVID with coagulation and complement comes from a genetic analysis of thousands of COVID patients from the U.K. Biobank, which contains medical records and genetic data on half a million people.
The authors found that variants of several genes that influence complement or coagulation activity are associated with more severe COVID symptoms that required hospitalization.
“These variants are not necessarily going to determine someone’s outcome,” Shapira says. “But this finding is another line of evidence that complement and coagulation pathways participate in the morbidity and mortality associated with COVID-19.”
Targeting Coagulation and Complement
Physicians treating COVID-19 patients have noticed coagulation issues since the beginning of the pandemic, and several clinical trials are underway to determine the best way to use existing anti-coagulation treatments.
Complement inhibitors are currently used in relatively rare diseases, but at least one clinical trial is testing the idea with COVID patients.
“I think our findings provide a stronger foundation for the idea that coagulation and complement play a role in COVID,” Tatonetti says, “and will hopefully inspire others to evaluate this hypothesis and see if it’s something that can be useful for fighting the ongoing pandemic.”
###
Reference: “Immune complement and coagulation functions in adverse outcomes of SARS-CoV-2 infection” 3 August 2020, Nature Medicine.
DOI: 10.1038/s41591-020-1021-2
Other authors: Vijendra Ramlall (Columbia University Irving Medical Center), Phyllis M. Thangaraj (CUIMC) Cem Meydan (CUIMC and Weill Cornell Medicine) Jonathan Foox (WCM), Daniel Butler (WCM), Ben May (CUIMC), Jessica K. De Freitas (Icahn School of Medicine at Mount Sinai), Benjamin S. Glicksberg (Icahn/Mount Sinai), and Christopher E. Mason (WCM.
This work was supported by the NIH (grants 5R01GM109018, 5U54CA209997, R35GM131905, F30HL140946, S10OD012351, S10OD021764, R21AI129851, R01MH117406, and R01AI151059), Scientific Computing Unit, XSEDE Supercomputing Resources, the Starr Cancer Consortium (I13-0052), WorldQuant Foundation, The Pershing Square Sohn Cancer Research Alliance, and NASA (NNX14AH50G, NNX17AB26G).
The authors declare no competing interests.